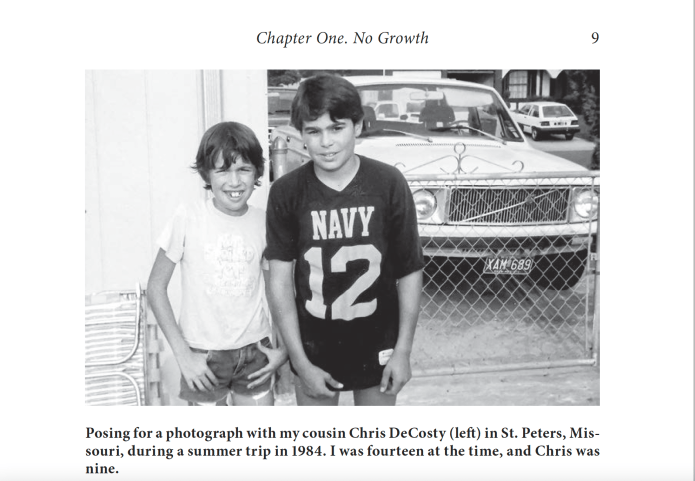
I’m brimming with gratitude for having wrapped up a great week. On Monday, Memorial Day, my memoir, Stunted: A Memoir of Delayed Manhood, was officially released by Toplight Books, an imprint of McFarland & Company. My Goodreads Giveaway continues until June 1 if you want to try to win a copy.
On Tuesday afternoon, I had my sixth-month follow-up appointment with my neurosurgeon, Dr. H. I received the radiologist’s report early Tuesday morning when I logged into Upstate’s patient portal. Upon reading that the tumor had grown measurably since the last scan in September, two thoughts swam through my brain—can the radiation oncology team hit the tumor with another round of Gamma Knife radiosurgery, and, if not, can I schedule my brain surgery over the summer so it won’t disrupt my busy work schedule that ramps up during the fall semester at Syracuse University?
To make it to my appointment, I had to take a Centro bus out to the Upstate University Medicine office in the Township 5 shopping center in Camillus, which is an Area 51-sized example of suburban sprawl.
Here are the quotes from the report that troubled me:
There has been “significant interval enlargement of the sellar and suprasellar mass consistent with known craniopharyngioma. On the current examination the mass measures 2.3 x 1.4 x 2.1 cm. On the comparison study dated 9/3/2025 the mass measured 1.6 x 1.1 x 1.7 cm.
“. . . There is worsened superior displacement and compression of the optic chiasm right worse than left.”
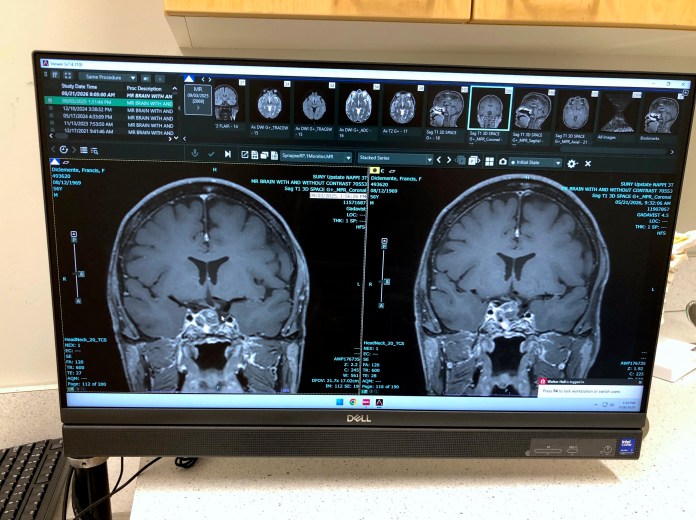
Yet when I see the always sanguine, gum-snapping Dr. H., he’s unruffled by the latest report. Dressed in a green, plaid flannel shirt and brown khakis, he takes a seat and explains that he reviewed the previous scans, lined everything up, and determined that the tumor has not grown significantly. He tries to allay my fears by giving me a detailed description of how different MRI machines or variations in the “slices of images” can affect the interpretation of the scan.
My two latest MRI scans appear on computer screens. The image on the left is from September, and the one on the right is from this May. The craniopharyngioma is the circular object in the middle of the brain.
Dr. H’s recommendation: Wait and see. Reschedule another MRI in six months.
I have no objection to this approach, and I left the office feeling grateful for another six-month reprieve—another half a year to live with no scheduled surgical intervention.
At the same time, I know the tumor isn’t sitting idle. It’s in a constant state of aggregation, growing steadily as the fluid inside expands, and at some point, it will likely provoke headaches and double vision (more than just to my extreme right).
But I try not to fall victim to the futility of worrying about my health (easier said than done).
##
On Friday, Upstate posted my conversation with host Amber Smith on the Informed Patient podcast. I much prefer pitching questions instead of fielding them.
I’ve conducted countless interviews in my role as a video producer at SU since 2007, and it’s definitely weird to be on the other side, to be the interviewee and not the interviewer. But it gave me a warm feeling of nostalgia for my radio days (circa 1996-2006).
My first shipment of books from McFarland & Company arrived yesterday. I’m so glad to see this book become a real thing—not just an idea in my head—because the project took more than 10 years to complete.
“Stunted: A Memoir of Delayed Manhood” is a coming-of-age story about identity and self-acceptance, told through the lens of my journey to adulthood after being diagnosed with a brain tumor when I was 15 years old.
The contains about 40 black-and-white photographs, medical records dating back to 1984, and diary entries from the early 1990s and beyond. It’s also loaded with sports and pop culture references from the ’80s and ’90s (e.g., Doug Flutie and The Cure).
I’m scheduled to give a reading at 6 p.m. on Tuesday, June 23, at Jervis Public Library in Rome, where, as a youth, I discovered my love of books and was introduced to authors such as John Steinbeck, Ernest Hemingway, Ray Bradbury, Albert Camus, Hermann Hesse, Joyce Carol Oates, and many others. I hope I won’t be so nervous that I ramble and babble.
A certificate for my participation in a summer reading program at Jervis Public Library in Rome in 1976.
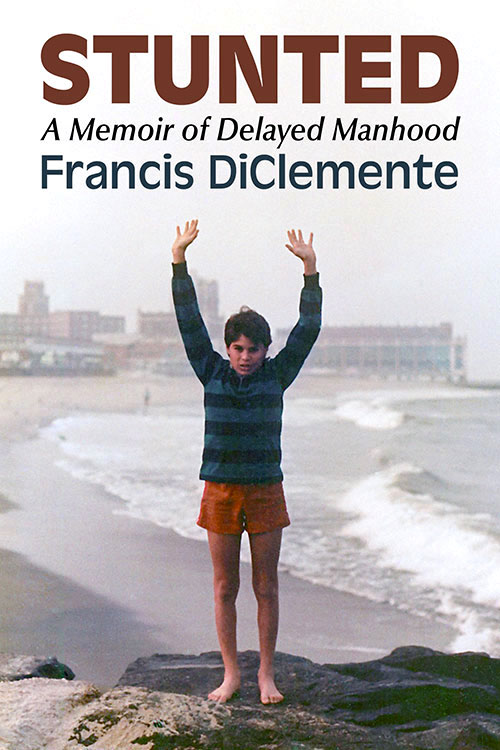
And I’m happy to share the cover image for my coming-of-age memoir, Stunted: A Memoir of Delayed Manhood, which is slated to be published later this year. It was a long, hard road to get here, but I am honored that the story has found a home with Toplight Books, an imprint of McFarland & Company.
I began researching this project in June 2013 after marrying my wife, Pam, who has been a steadfast supporter, cheering me on along the way. I obtained medical records dating back to 1984 and incorporated journal entries from the early 1990s. So in many ways, I’ve been writing this memoir my whole life. The impetus to write the book sprang from a long blog post I wrote in December 2014 to mark the 30th anniversary of my initial brain surgery at SUNY Upstate Medical University Hospital in Syracuse, New York.
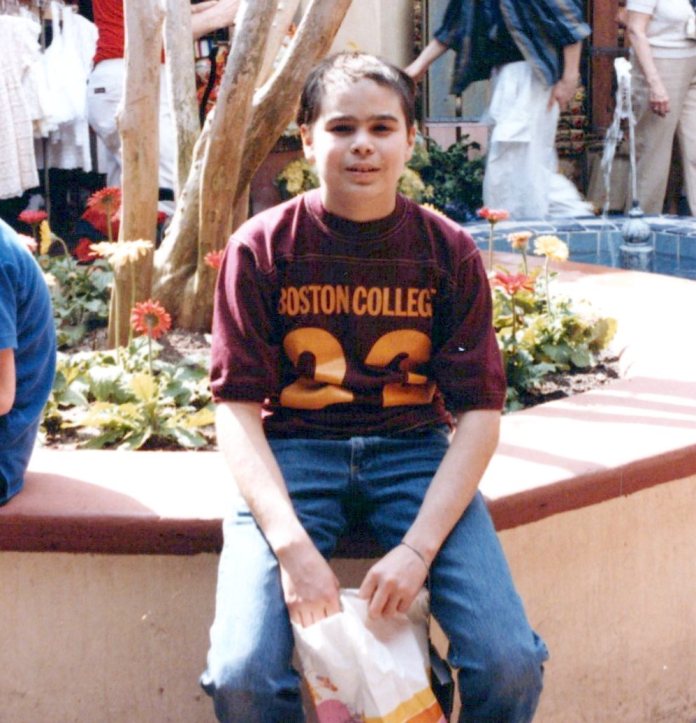
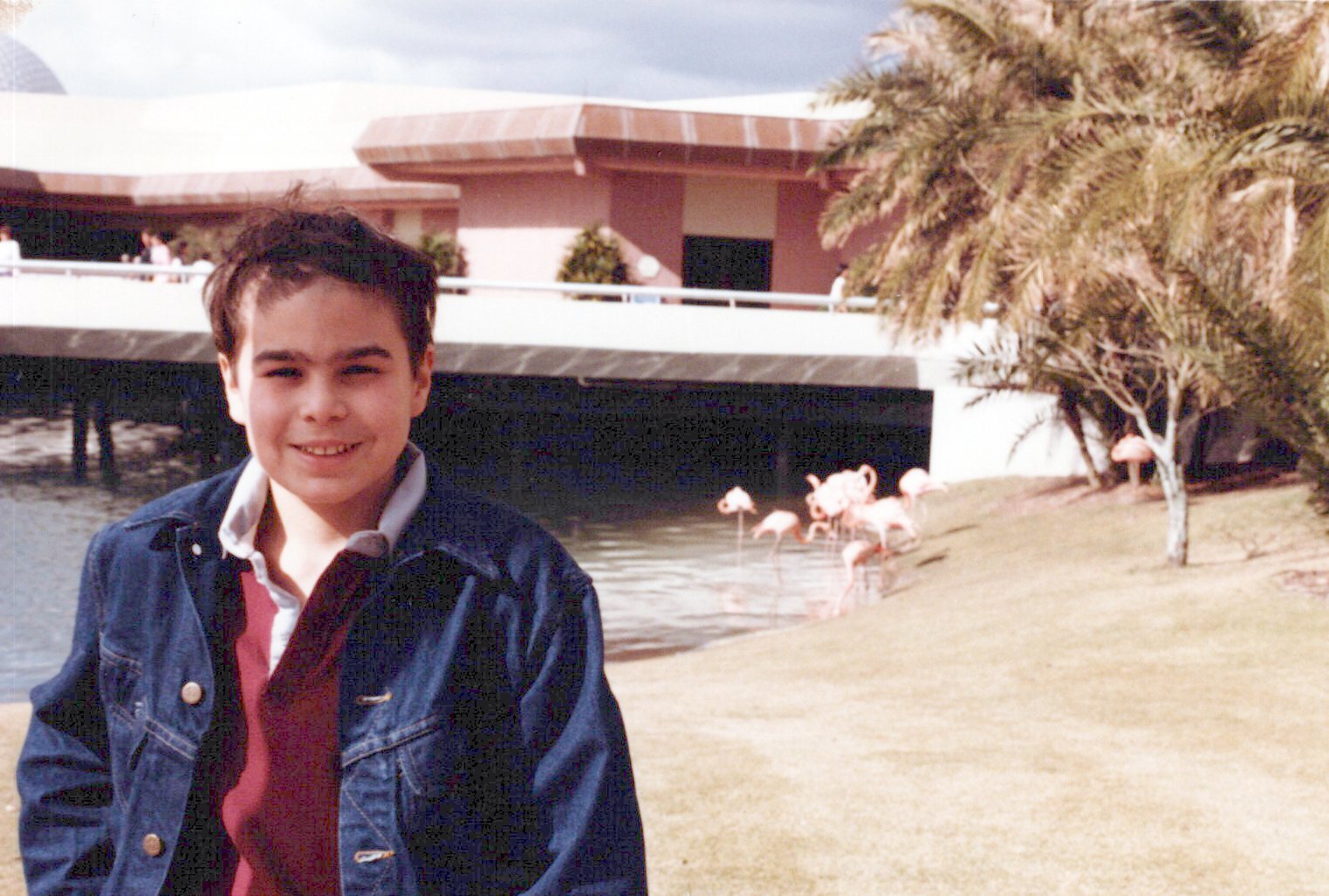
At Walt Disney World in 1985, a few months after my initial brain surgery.
When I started working on the memoir, I realized I needed to study the genre, so I read the classics like Angela’s Ashes by Frank McCourt, The Liars’ Club by Mary Karr, This Boy’s Life by Tobias Wolff, Running with Scissors by Augusten Burroughs, Wild by Cheryl Strayed, Stop-Time by Frank Conroy, Eat, Pray, Love by Elizabeth Gilbert, I Know Why the Caged Bird Sings by Maya Angelou, and many, many others.
Between that initial blog post and the completion of the book, life intruded.
I had two brain surgeries, was diagnosed with rheumatoid arthritis, mourned the loss of my stepfather, Bill Ruane, my Uncle Fiore DeCosty (nicknamed Fee), and two cousins, Derek and Damon DeCosty. I published numerous poetry collections, wrote a play that was produced by a small theater in Las Vegas, produced a few documentary films, and earned two Emmy awards. I bought a house (reluctantly), and most importantly, became a father to my son, Colin, who will be ten years old next month and was diagnosed with autism in 2018.
The whole time I was living my life in the present while my head remained partly stuck in the time period from 1984 to 1995, covering the terrain of my high school experience in Rome, New York, my undergraduate years at St. John Fisher College (now named St. John Fisher University), in Rochester, New York, graduate school at American University in Washington, DC, and the start of my professional career back in my hometown of Rome and in Venice, Florida.
Here’s me in either my junior or senior year of high school or my freshman year at St. John Fisher College in Rochester, New York.
And as time elapsed and I wondered if I would ever finish the book, I drafted scenes, wrote a crappy first draft, completed multiple revisions on my own, and then hired developmental and line editors through Fiverr, wrote a book proposal, and sent out countless queries to agents and publishers who accept direct submissions from authors.
While I am ecstatic that the book will be published, I detest the necessity of the promotional phase. But it’s a reality I can’t escape. My intention is for readers to find some universal truth or connection to my personal story.
Here is the book description from the McFarland site.
Set between 1984 and the mid–1990s, this coming-of-age memoir follows Francis DiClemente’s experience of adolescence and early adulthood in a body that struggled to develop. Diagnosed with a rare brain tumor that led to hypopituitarism, DiClemente remained physically underdeveloped while his peers matured into young adulthood. As he navigated relationships and sexuality in college, it became evident that his prolonged experience with physical nonconformity fueled isolation, self-doubt, and shame.
This book explores the impacts of his condition on schooling, intimacy, and emerging adulthood, examining how physical differences shape identity formation. It reframes masculinity not as a function of physical development, but as an ethical and emotional practice grounded in empathy, resilience, and responsibility. Contributing to conversations on embodiment and self-acceptance, the work offers insight into the experience of living at odds with normative timelines of growth and belonging.
And I was very fortunate to have some gifted and generous writers provide blurbs for marketing.
“Francis DiClemente’s searingly honest memoir offers a vital perspective for anyone grappling with their own place in the world.”
—Shivaji Das, author of The Visible Invisibles
“Francis DiClemente and I met as teenagers on a baseball diamond in the summer of 1983, and while I have since gone on to work in a different sport populated by alpha males gifted with superhuman size, strength, and athleticism, I know of no better or stronger example of what manhood truly means than my friend. This moving story of self-discovery, which Francis courageously tells with raw honesty and vulnerability, reminds us that the journey toward fulfillment in life is inward, and should inspire us to be less judgmental—not only of others but ourselves.”
—Bob Socci, broadcaster, New England Patriots
“DiClemente’s journey becomes a lifelong battle, man against regrowing tumor. In these pages, he provides the most intimate details of how he learned to be a man while trapped in the body of a boy. Hopefully, his words, and his honesty, can reassure other boys and men grappling with masculine identity.”
—Angel Ackerman, author of the Fashion and Fiends horror series and founder of Parisian Phoenix Publishing
“This is a deeply moving testament to the quiet courage it takes to claim your identity in a world that insists on defining it for you. For anyone who has ever felt unseen or out of place, DiClemente offers a reimagined vision of identity rooted not in the body, but in the soul.”
—Brittany Terwilliger, author of The Insatiables
“Francis DiClemente has written a book on men and masculinity that should be not only savored but consulted by those men who, at some point in their lives, have questioned what their manhood means and what place it holds in society. And by those men I mean all men. This work might have been born of DiClemente’s many masculine hardships, but it becomes a celebration of what is best in us.”
—William Giraldi, author of The Hero’s Body
“DiClemente delivers an unflinching account of the brain tumor that disrupted normal growth and his participation in one of the first human growth hormone trials. …a touching and compelling memoir.”
—Carmen Amato, author of the Galliano Club historical fiction series
“Francis DiClemente tells it like it is—with no BS. This work is honest, human, and full of hope. I respect the courage it took to write it.”
—William Soldato, author of Under Too Long
“Francis DiClemente’s book is a courageous and beautifully crafted memoir that speaks to the quiet battles so many face in silence. With poetic clarity, brutal honesty, and emotional depth, he explores identity, masculinity, and the long road to self-acceptance. A powerful book.”
—Apple An, award-winning author of Las Crosses, Mother of Red Mountains, and Daughter of Blue City
I’m now working on a second book, which is a continuation of the story. There’s no timetable for completion.
One note about the cover.
My Uncle Fiore took my photo in 1985 at the New Jersey shore. We had traveled to New Jersey from Rome one early fall weekend to visit my cousin, Fiore, who was stationed at an Army prep school in Monmouth County, where he would spend a year before matriculating to the U.S. Military Academy at West Point. I remember listening to Bruce Springsteen’s Born in the U.S.A. album on my yellow Sony Walkman in the backseat on the way down from Rome to Jersey. I connected the song “I’m Goin’ Down” with our southbound travel, and I loved side two of the album, especially the songs “No Surrender,” “Bobby Jean,” and “My Hometown.”
During a recent appointment at the Nappi Wellness Institute at SUNY Upstate Medical University Hospital, I saw this impressive mural by Japanese artist Tomokazu Matsuyama.
Solitude Aqua Amore, 2023 by Tomokazu Matsuyama.
I’ve written about the soothing effect of hospital art before. A few years ago, a framed print in an MRI waiting room inspired this poem, which was published in my 2021 collection, Outward Arrangements: Poems.
Waiting with Vincent
A scheduled MRI
of the brain shifts
my thoughts toward
all of the
“what if, worst-case scenarios.”
While waiting for my name
to be called,
I see a print of Irises (1889)
hanging on a wall.
From far across the room,
without my glasses,
the slanted vertical
green leaves
look like snakes
writhing in the dirt.
But the longer
I stare at the image,
the calmer I feel. Placid is the word
that comes to mind.
And I’m thankful Vincent
spends a few
moments with me
prior to my appointment
with the tube machine.
Because when sitting
in a hospital
waiting room,
artwork by Vincent
never fails to lift the spirits.
A van Gogh painting beats People magazine
or an iPhone screen
every time.
The mural is entitled Solitude Aqua Amore, 2023, and Matsuyama worked with the nonprofit organization RxART, which “pairs leading contemporary artists with pediatric hospitals to develop site-specific projects that humanize the healthcare environment and improve the patient experience.”
I think it’s a wonderful concept, and I have no doubt that colorful artwork in hospitals lifts the spirits of little patients and their parents during their tense moments (or hours) of testing, waiting, and meeting with doctors and medical staff.
The RxART website displays images of completed projects at hospitals across the country.
I like the close-up iPhone photo I took because it put me smack in the middle of the painting, and the detailed image made me think of a Jackson Pollock drip painting—but featuring birds.
Detail image of Solitude Aqua Amore, 2023.
Here is the wall text for Matsuyama’s piece:
Tomokazu Matsuyama Solitude Aqua Amore, 2023
Courtesy of the Artist
“Tomokazu Matsuyama is a contemporary artist who is keenly aware of the nomadic diaspora, a community of wandering people who seek to understand their place in a world of contrasting visual and cultural dialects. Tomokazu has created this bright and uplifting imagery to transform the institute’s International department. This work, inspired by “a thousand origami cranes,” encapsulates the essence of hope, peace, and the mythical attributes of good fortune. Utilizing geometric forms and organic curves, he weaves the inherent desire associated with the ‘senbazuru’ tradition into a narrative that resonates with the contemporary era. Tomokazu was born in Takayama, Gifu, Japan, and lives and works in Brooklyn, NY. RxART is grateful to Chris Salgardo, ATWATER, and Ducati for lead support of this project.”
Side note: These days, it seems whenever I read biographical text about a writer, poet, filmmaker, or artist, the bio invariably ends . . . “[Insert artist name] lives and works in Brooklyn, New York.” And that makes me wonder if poems are flying through the air and paint is flowing in the streets of Brooklyn. If I ever get to New York again, I’ll need to make my way there to explore the scene.
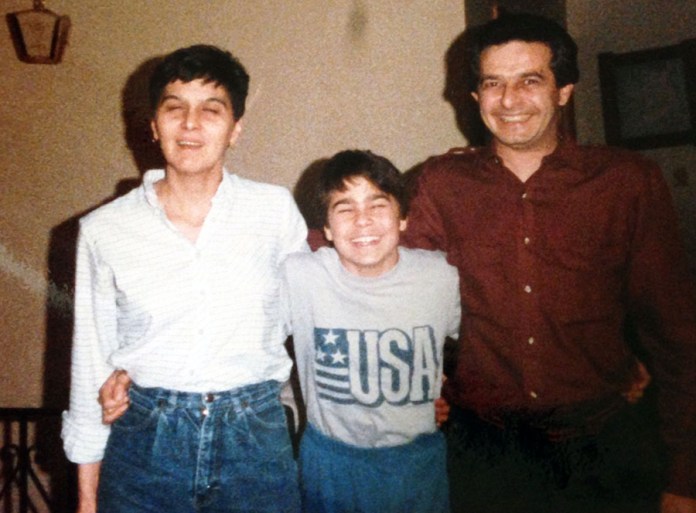
Today marks the forty-first anniversary of my first brain surgery. As I’ve written about before, on Dec. 12, 1984, when I was fifteen years old and a sophomore in high school, surgeons at SUNY Upstate Medical Center (now named Upstate University Hospital) in Syracuse, New York, removed a large craniopharyngioma that had engulfed my pituitary gland, leading to stunted growth and delayed puberty. Since then, I’ve had four additional surgeries and two Gamma Knife radiosurgery treatments at Upstate.
Posing with my parents prior to my surgery in 1984.
Prior to the initial surgery, in the fall of 1984, a scan of my head had revealed a cloudy mass in the sella region at the base of the skull, and the results of a follow-up CT scan with radiation contrast came a few weeks later.
I received the news about the brain tumor diagnosis from my father when he picked me up from wrestling practice on a cold November night. This essay describes that encounter.
Craniopharyngioma
##
After I put on my black wool pea coat, pulled a knit hat down around my ears, and slung my book bag over my shoulders, I pushed open the back door of the gym and walked outside to meet my father, who had parked behind the high school.
The cold air hit my face and stung my gloveless hands as I strode toward the car; a floodlight cast a large net of bright, white light on the pavement. Dad drove up, and I got in.
He left the car idling, and as I slid into the passenger seat and adjusted myself, he leaned over and kissed me on the cheek, his tan winter coat brushing against the steering wheel. I felt a trace of his beard stubble against my skin, and I could smell a faint odor of Aqua Velva or Brut combined with cigarette smoke. The heater hummed, and he lowered the blast of air and turned and looked at me. I wondered why we weren’t moving yet. He wasn’t crying, but he appeared on the verge of spilling emotions.
“What’s the matter, Dad?” I asked.
“Upstate called your mother today,” he said. He switched on the overhead light, reached into his jacket pocket, and pulled out a torn piece of paper. “Here,” he said, handing me the slip of paper, “this is what they think you have. I wrote it down, but I don’t think I spelled it right.”
In a slashing style in faint, blue ink, my father had scribbled a misspelling of the word craniopharyngioma. His voice cracked as he said, “It’s cranio-phah-reng . . . something like that . . . oh, I don’t know. It’s some kind of brain tumor.”
I looked at the paper as my father let out a sigh. He shook his head and said, “I prayed to God when you were born that this wouldn’t happen to you, that you wouldn’t have to go through the same thing I did.” His words referred to his health crisis as a teenager, one that caused small stature and delayed puberty and led to ridicule by his classmates.
Francis DiClemente Sr. was born with a hole in his heart, a ventricular septal defect. On June 12, 1959, when he was sixteen years old, pioneering cardiac surgeon C. Walton Lillehei performed open-heart surgery on him at the University of Minnesota Hospital, successfully repairing the defect.
The heart problem disrupted Dad’s high school years, and he faced a long recovery; but he rebounded after the surgery, lifting weights to become stronger and adding muscle to his thin frame. He grew to his final adult height, graduated high school from St. Aloysius Academy in Rome, and went to work at the city’s Sears Roebuck store.
After sharing the information with me, he pressed his lips together and shook his head again, and he seemed locked in position in the driver’s seat, unable to contend with the news, incapable of going through the motions of driving away. We clenched hands, and I said, “It’s OK, Dad. Don’t worry. But what do we do now? What’s next?”
“You have to go back there for more tests. You may need surgery.”
“All right,” I said. “It’s OK.”
“I hope so,” he said. “All we can do is pray.”
He switched off the overhead light, put the car in drive, and drove out of the parking lot. We grew silent as we passed the naked trees lining Pine Street in our city of Rome, New York.. We crossed the intersection at James Street and made our way toward Black River Boulevard.
While my father was anxious and crestfallen, I felt elated as I gripped my book bag in the passenger seat. The CT scan with contrast had confirmed my suspicions, indicating a grave medical condition was responsible for my growth failure at age fifteen, offering a reason why my body had not changed, why I had not progressed through puberty, and why I remained so different from the other boys my age. I still considered myself a physical anomaly, but the tumor proved it wasn’t my fault.
I looked down at the piece of paper again and studied the word. Craniopharyngioma. I tried to sound it out in my head while my dad steered the vehicle, and I thought the word would twirl off my tongue like poetry if I rolled down the window and yelled it. Craniopharyngioma. Cranio-Phar-Ryng-Ee-Oh-Mah. It reminded me of onomatopoeia, which I had learned about in my tenth-grade English class.
##
And here are two related poems:
Case History
Stricken with pituitary insufficiency,
I felt my way through
a stage of delayed puberty.
When adolescence took hold for other kids,
I remained like a boy wrapped in toddler’s clothes.
My face looks older now,
and my body has grown.
But I could not escape
the endocrine impact of that cranial intrusion.
For even though benign,
the tissue overtook me,
and in effect, the tumor
scarred my life and altered my future.
Craniopharyngioma (Youthful Diary Entry)
Craniopharyngioma gave me
an excuse for being unattractive.
I had a problem inside my head.
It wasn’t my fault
I stood four foot eight inches tall
and looked like I was
twelve years old instead of eighteen—
and then nineteen
instead of twenty-four.
I couldn’t be blamed for
my sans-testosterone body
straddling the line
between male and female.
The brain tumor
spurred questions
about my appearance,
aroused ridicule,
and provoked sympathy.
I heard voices whispering:
“Guess how old that guy is?”
And, “Is that a dude or a chick?”
And while I waited for my
body to mature, to fall in line,
and to achieve normal progression,
I remember wishing the surgeons
had left the scalpel
inside my skull
before they closed me up,
knitting the stitches
from ear to ear.
I prayed the scalpel
would twist and twirl
while I slept at night—
carving my brain
like a jack-o’-lantern—
splitting the left and right
hemispheres,
and effacing the memory
of my existence.
Two years ago today, I underwent my sixth brain surgery at Upstate Medical University Hospital for a recurring benign tumor on my pituitary gland. A neurosurgery and ENT team removed the stubborn craniopharyngioma in a four-hour surgery on July 24, 2023.
Upstate Medical University Hospital (Photo by Francis DiClemente)
I wrote a poem based on the postoperative medical report uploaded to the MyChart portal. I consider this a “reverse redacted poem.” Instead of blacking out words from my source text, I pulled words and phrases from the summary.
Neurosurgery Report
Date of Procedure: July 24, 2023
Endonasal endoscopic
transsphenoidal resection
of tumor
with nasal septal flap.
Preoperative diagnosis:
Recurrent craniopharyngioma
Postoperative: Same
Patient is a 53-year-old male
with a long history
of known craniopharyngioma.
Recurrence of craniopharyngioma
abutting the optic chiasm.
Not a great candidate
for repeat radiosurgery—
not enough margin
between the tumor
and the optic chiasm.
Counseled on the risks
and benefits of endonasal
transsphenoidal resection.
Elected to proceed
despite the risks.
Patient was intubated
by anesthesia.
Positioned supine
with the bed turned 90 degrees.
Endonasal approach
to the sphenoid sinus.
Once the sella was exposed
and the bone drilled down,
we began our resection.
A long handled arachnoid knife
was used to incise the dura.
The tumor was located
mainly on the right side.
We then encountered
thick scar tissue,
which was also incised
in cruciate fashion.
Once both layers of dura
had been opened,
there was immediate egress
of thin viscous brown fluid.
With the endoscope
we could see a
calcified appearing tumor
just in front of our field.
At this point, there was a brisk
CSF (cerebrospinal fluid) leak
from the chiasmatic cistern most likely.
Once we had attempted
to scrape along the floor
of the sella posteriorly and laterally
along the cavernous sinus,
we then turned our attention
to the tumor hanging in front of us.
We used laryngeal biopsy forceps
to coax the tumor out.
At this point, the tumor
seemed fairly stuck and plastered
to the arachnoid superiorly,
and thus we resected the
remaining tumor in front of us
in piecemeal fashion.
Given the brisk CFS leak,
our ENT colleagues then turned to
the right-sided nasal septal flap.
The ENT repaired the CSF leak.
Packing Surgical and NasoPore dressing
placed by the ENT surgeons.
This concluded our procedure.
The drapes were then removed.
The patient was returned to the stretcher.
He was successfully extubated
by anesthesia and transported
to PACU (Post Anesthesia Care Unit)
in stable condition.
Now, two years later, I am still living with a brain tumor. My last MRI in December 2024 revealed:
“The lesion measures 14 mm x 13 mm (TV by AP; Transverse by Anteroposterior), unchanged compared to prior scan dated 5/17/2024, allowing difference in technique and slice selection. The superior aspect of the mass abuts supraclinoid ICA, which remains patent. The right prechiasmatic optic nerve demonstrates mild atrophy but remains unchanged.”
My next MRI is scheduled for September. I suffer some mild headaches and have double vision when looking at a computer screen without my prism prescription glasses or gazing to the extreme right. But otherwise, the tumor is not affecting my health.
And I know what Dr. H. will say when he reads the MRI report in September. He’ll say, “Your scan looks good. It hasn’t grown. Let’s leave it alone and get another MRI in six months.”
This wait-and-see approach works well for me. But at the same time, I can never get the tumor out of my head—literally and figuratively.
And although Dr. H. is the surgeon and I respect his medical advice, his Pollyanna outlook ruffles me.
That’s because Dr. H. isn’t troubled by a repetition of sneezes that I fear could dislodge the tumor from its nook and cause it to invade healthy brain tissue. Dr. H. doesn’t worry that eating an entrée of fish and chips will add protein and fat to the tumor cells and make the mass larger. He’s not worried that the tumor will expand and start pressing against the optic nerve.
Craniopharyngiomas consistently grow back; that’s their nature. Having this dormant beast taking up real estate inside my skull feels like having Godzilla asleep in your cellar. You know he’ll wake up eventually. And then what? So how can you sit at the kitchen table and blithely enjoy a quiet dinner when you know the predator lurks beneath your feet?
At the same time, life and death could trade places on any given day. I’ve lost two cousins younger than sixty years old in the past six months (Derek DeCosty and Damon DeCosty), and I know tomorrow is not guaranteed. I am also very fortunate not to have a malignant tumor or a fatal disease.
And since I have no alternative, I live with the tumor as best as I can and try to forget it’s still there. Meanwhile, the tumor remains in the act of waiting—waiting to decide what it will become, waiting to find its path, waiting to strike. The neoplasm’s presence inside my head troubles me if I allow the image of the fluid-wrapped mass to provoke my worst fears. But for now, I try not to disturb the sleeping beast.
I received a nerve conduction study last week related to symptoms of my rheumatoid arthritis. The bearded electromyography (EMG) technician, Mark, had dark hair and an athletic build, and he wore glasses. We made small talk while he placed electrodes on me, stimulated the nerves with mild electrical shocks, and measured the results on a computer.
When I asked him where he was from, he said he grew up in Syracuse and went to a local high school. “It was a really good school,” he said, noting its academic and athletic excellence. “But I didn’t appreciate it at the time. I was kind of a screw up.”
He also explained that his mother was a custodian at Syracuse University and how he could have gone to college there for free, but didn’t take advantage of the opportunity. “I blew it,” he said. “But I had to find my own way.”
And then he said a jewel of a statement regarding regret. “If you focus too much on regrets, you don’t appreciate the life you currently have.” Or he may have said, “If you focus too much on regrets, you don’t live the life you currently have.”
Regret is a recurring theme in my poetry. I think it’s something all adults at a certain age wrestle with—this idea of ambitions versus reality.
Camera Angle
What would I choose
if I were given a chance
to lead a different life?
What mistakes
would I correct?
What new road
would I take?
But you can’t splice
the scenes of your life
to edit the past.
You can only point
the camera forward
and zoom into the future.
I am celebrating an important milestone today—the 40th anniversary of my first brain surgery to remove a benign tumor engulfing my pituitary gland. I have written about this ordeal many times in the past, including in this long 2014 post.
On this day, four decades ago, surgeons cracked open my skull and extracted the craniopharyngioma that had stunted my growth and delayed my transition from boy to man.
In this essay, I reflect on my experience as a teenager in 1984 while a patient at SUNY Upstate Medical Center (renamed Upstate University Hospital) in Syracuse, New York. I am limiting the narrative period to the day of surgery and my immediate recovery.
Upstate University Hospital
Surgery Day: An Essay
1.
Early morning. Blackness. I can smell the breakfast trays delivered on the hospital floor—watery eggs, ham and bacon, soggy oatmeal, and weak tea and coffee. The noise outside my room grows as patients awaken and nurses draw blood and administer medicine.
My appointment with the medical intervention team has arrived. I am fifteen years old and ready for surgery day, prepared for the trauma that awaits me on the table. My head will be shaved, and my skull sawed open. The tumor growing in my head—wrapped around my pituitary gland and stifling my maturation—will be plucked free, yanked out like an infected molar and then examined under a microscope to determine its classification. We must name our enemies to defeat them.
Once removed, the lesion will relinquish dominion over my body. I will be cut loose from its tentacles. The surgery will disrupt my endocrine system, leading to a permanent condition known as hypopituitarism and propelling me on a long road toward “catch-up” growth and development.
A photo of my father and me two months before the operation in 1984.
2.
A nurse enters my room and hands me a small plastic cup filled with a few pills. “This will just relax you,” she says as I swallow the pre-surgery drugs. About a half-hour later, she returns and says, “It’s time for you to go down now.” A softness squishes against the edges of my mind; I am drifting from consciousness.
An orderly comes to take me away—filling nearly the entire space inside the door frame. A hulking figure with thick, black hair, a black beard, and muscular forearms, he reminds me of Bluto from the Popeye the Sailor cartoons. But for some reason, I call him Hugo.
“OK, Hugo,” I say, “I’m ready now.” Hugo helps me slide over from my bed to a stretcher as the nurse covers me with a sheet and a blanket.
My family gathers around me, bending down to kiss me and wish me “good luck.” What does “good luck” mean on the operating table? I wonder.
Tears stream down my mother’s cheeks, which are red and wind-burned and feel cold against my skin as she kisses my face and forehead; she squeezes my hand and then releases her grip and steps away.
Hugo unlocks the wheels of the gurney and steers it out of the room and into the hallway. Even though I am sleepy, I stay awake for the ride, keeping my eyes open and watching the panels of fluorescent lights pass overhead as we make our way through the hospital corridors and into an elevator. We take a silent ride down to the surgical wing.
The temperature drops when we enter the frigid, sterile operating room. A chill runs over my body; my lips tremble as gooseflesh buds on my arms.
The surgical team members buzz around the operating room, each doctor or nurse carrying out a specific task. They transfer me from the stretcher to the operating table. An overhead light shines into my eyes while I lay splayed on the table.
A nurse covers me with an extra blanket and stretches tight, white stockings over my calves. She says the stockings will help to prevent blood clots after surgery.
One of the doctors sits down near the table and says he will shave my head. When he asks me if I want my whole head sheared or just the front, I make the mistake of telling him to clip only the front. As a result, weeks after the surgery, my hair remains uneven—bald in front and growing long in the back—similar to the long hair sticking out the back of helmets worn by hockey players with mullets.
After they jab an IV in my arm, I grow drowsy, my eyelids shutting; but before I drift off, I tell one of the nurses that I need to pee. The woman chuckles and says, “Oh, you don’t have to worry about that now. We’ve already put in a catheter.”
And then I leave the world—falling under the power of general anesthesia for about eight-and-a-half hours while the surgeons perform their work.
At Walt Disney World in February 1985.
3.
I have often wondered where I traveled to during that gap of time. What realms or landscapes did I explore in my mind while my skull lay open and I remained unconscious on the operating table?
Here is me stepping out of the story momentarily to travel back in time and investigate the scene. It’s a fantasy of the man I hoped I would become once the surgeons extracted the tumor. It’s the future I had envisioned for myself—marked by maturation and normalcy, playing the role of a fully formed male accompanied by a female partner.
A green canopy of trees. A trilling stream. Sunlight filtering through leaves overhanging a hiking path. Birds chirp, and tree limbs sway in the wind.
Boots touch the soft, muddy earth. A man emerges from a wooded path. He is dressed in a red checkered flannel shirt, tan khakis, and hiking boots, and he carries a knapsack on his shoulders. He is about five feet six inches tall, lean and muscular, and has a slight beard.
A twig snaps, and we see a woman walking out of a clearing. She’s wearing a fleece sweatshirt, jeans, hiking boots, and a backpack. The two figures stride toward one another, share a kiss, and then grasp hands. Sunlight bathes them as they leave the clearing and start walking on a path leading over a ridge. They climb the slight incline and disappear as they walk down the other side, their bodies concealed by the curve of the Earth.
Late high school or early college years.
4.
I wake up in a bed tucked in a corner of the surgical intensive care unit. I feel dizzy, and a dull, continuous ache presses against my head as if my skull is being squeezed in a vice. Nurses inject the opioid Demerol into my thighs over several hours to alleviate the pain, and I keep drifting in and out of sleep. I hear machines beeping and the sound of a respirator somewhere on the floor. The gentle sound of the ventilator puts me at ease as I listen to it—in and out, in and out, in and out.
EKG stickers are pressed to my chest, and machines monitor my heart rate and blood pressure. Vaseline has been smeared on my eyelids and eyelashes, clouding my vision, and I feel like I am straining to see from under the cover of a heavy, wet blanket. The white stockings the surgical team had given me are pulled up to my knees and constrict the circulation in my lower limbs.
I feel small—shriveled up in the bed like a green-gray alien being prodded by U.S. government doctors and scientists on an operating table in Roswell or Los Alamos, New Mexico. A scar runs the entire length of my head, from the tip of my right ear to the tip of my left ear. I tap a slight dent in my skull (produced by a right frontal craniotomy during surgery), about the width of two fingers, just above my forehead on the right side.
The stitches itch, and I reach up to feel the thick, black threads. I wonder if I resemble a twisted version of the Mr. Met mascot.
5.
But I feel relieved because I have awakened from the operation, and my brain function remains intact. Some doctors lean over my bed and ask me a series of questions: Do I know my name, the current year, the president of the U.S., and the name of the city I am in? I answer the questions correctly, and when instructed, I squeeze their fingers, wiggle my toes, puff my cheeks, stick out my tongue, and follow a penlight with my eyes.
My senses function properly, as I can see, hear, speak, and smell. I can form thoughts, and the trauma of the surgery has not altered my mental ability or effaced my memory.
My mother, father, sister, and Aunt Teresa huddle around my bed, their faces beaming like those of Dorothy’s relatives in the scene when she wakes up from the dream at the end of The Wizard of Oz.
“Hey, buddy,” my dad says.
My mom leans over the bed rail, kisses my face and eyelids, and says, “You did great, honey, just great.”
“Yeah, Dr. B. said he got most of it,” Dad says.
“Was it big?” I ask.
My mom holds up her right thumb, indicating the size of the tumor. “It was about the size of a thumb,” she says. She caresses my face and adds, “Dr. B. said there’s a little bit left over, but we don’t need to worry about that now.”
“OK,” I say, closing my eyes and returning to sleep.
High school graduation in 1987.
6.
I wake up on the first night with a raging thirst in my parched throat. I feel like I have been deprived of water for days. But because the doctors are concerned about swelling in the brain, they load me with corticosteroids and restrict my fluid intake. My face is swollen, and I feel bloated from the steroids; I am not allowed to drink water, but I am permitted to suck on ice chips.
However, late in the evening, with the lights dimmed on the floor after visiting hours have ended, I turn my head, look around, and notice a sink in the corner, only a few feet away from my bed.
Somehow, despite being woozy, I lower the bed rail, swing my legs out to the side, and climb out of bed. I try to be quiet as I wheel my IV stand toward the small, stainless-steel sink. I turn on the foot pedal faucet, cup my hands, and gulp the water like it’s rushing in an icy mountain river.
The cold liquid pours down my throat and gives me immediate relief. I want to stay here and drink more water, but a man—a male nurse or an orderly—races toward me and pulls me away from the sink.
“What are you doing?” he yells. “You just had brain surgery.”
He then escorts me back to bed, swings my legs over, covers me with the blankets, and lifts the bed rail.
“Now, don’t get up again,” he says. “What do you wanna do, crack your head open and screw up the work those surgeons did?”
And now tucked back into bed, I resume sleeping, drifting off until the next wave of pain hits, and I press the call button to request another dose of Demerol.
##
Recalling these past forty years, I run a tally of my surgeries at Upstate. The number stands at six—counting the initial surgery in 1984 and the subsequent operations to remove tumor regrowth in 1988, 2011, 2012 (Gamma Knife), 2020 (Gamma Knife), and 2023.
I have some double vision when looking at things up close and to my extreme right (right sixth nerve palsy), and I must be hyper-vigilant in the management of my care to treat my hypopituitarism. But except for my corticosteroid-induced osteoporosis and rheumatoid arthritis (unrelated to the tumor), I am a healthy, middle-aged man.
My next MRI is scheduled for Dec. 18. And with the stubborn resilience of craniopharyngiomas, I know more surgeries (or radiation treatments) loom in the future. But I face each day with gratitude, recognizing how lucky I am to have survived the scalpel on multiple occasions. I also don’t look beyond each six-month window of time between MRIs. Once my current neurosurgeon orders the next MRI, I go about my life without thinking about the tumor still lurking in my head.
Late high school or early college years.
##
And because of the significance of the number 40 on this anniversary date, I’ll leave you with U2 playing “40” live at Red Rocks Amphitheatre in Colorado in 1983.
One year ago today, a neurosurgery and ENT team at Upstate University Hospital took a nasal approach to remove the remnants of a craniopharyngioma (a benign tumor on the pituitary gland). It marked my sixth brain surgery since age 15.
I have fully recovered from the surgery, resuming all activities, although I still suffer occasional bloody noses and have peripheral double vision (which is likely permanent).
Photo of me last summer, after my surgery.
Vestiges of the tumor—what my neurosurgeon calls “membranes and scar tissue” still reside inside my head, as outlined in my latest MRI report:
FINDINGS:
“. . . In the right paramedian aspect of the surgical bed in the sellar/suprasellar region again seen is mass with heterogeneous enhancement which measures approximately 1.2 x 1.4 cm by my measurements.”
For now, the mass “remains grossly unchanged,” but the nature of craniopharyngiomas means the tumor will likely grow back to a point where another surgery or radiation will be required.
However, my medical condition is not the subject of this post. I just needed a brief introduction with a reference to the anniversary of my surgery.
Instead, I want to share some musical selections I listened to in the days and weeks following my surgery last summer. These songs aided me, providing succor while I recovered, propped up in bed, unable to sneeze or blow my nose, and moving gingerly around the house.
As I listened to the songs, I reflected on my life, swelling with gratitude for being alive and making gradual progress—supported by my wife, Pamela.
I think the tunes can provide positive affirmation for anyone facing adversity.
“I’m Still Standing” by Elton John
“Winning” by Santana
“Back in the High Life Again” by Steve Winwood
“Better Days” by Bruce Springsteen
More about Bruce later . . .
As someone who grew up in the 1980s, I am mesmerized by the concert footage available on YouTube. It is amazing to think you can see bands performing in 4K (some clips with multicam edits) hours after a show. When I was a kid, I listened to 95X in Syracuse after a concert by the Rolling Stones at the Carrier Dome so I could hear the DJ run down the setlist.
During The Cure’s 2023 North American tour, they played five original songs that I believe will be included in their forthcoming album, Songs of a Lost World. Two of my favorites from the new batch are “Alone” and “Nothing is Forever,” which I listened to repeatedly during my recovery. They put me in a dreamy headspace where I could forget about my health problems.
“Alone” by The Cure
“And Nothing is Forever” by The Cure
I also turned to the Grateful Dead for repeat listening during the late summer of 2023—often clicking on two tracks from the Dead’s famed 1977 concert at Barton Hall at Cornell University.
“Morning Dew” by the Grateful Dead
“Terrapin Station” by the Grateful Dead
And finally, there’s Bruce.
Bruce Springsteen and the E Street Band were initially scheduled to perform at the JMA Wireless Dome in Syracuse in early September 2023, but the show was canceled because of Bruce’s peptic ulcer disease. It was fortunate for me because I would have been in no condition to climb the concrete steps to the upper rafters of the Dome just a few weeks after brain surgery. But I attended the rescheduled show in April 2024, and I’ll leave you with “Backstreets” (which references summer).
“Backstreets” by Bruce Springsteen and the E Street Band
Today marks nine months since my surgery to remove a benign brain tumor on my pituitary gland. Although it’s not a major milestone, it’s tied to a once-in-a-lifetime event—seeing Bruce Springsteen in concert on April 18 in the JMA Wireless Dome in Syracuse.
The concert was originally scheduled for September 7, 2023, and I would have been in no condition during my recovery to climb the concrete steps to the upper rafters of the Dome in Section 336, Row Y. I transferred my ticket to a co-worker, but then the tour was sidelined due to Bruce’s peptic ulcer disease. I’d like to think some heavenly intervention permitted me to attend the rescheduled event in April in a fully restored state.
I went to the concert with my wife, Pam—a rare night out for us and a break for her as she completed her first full year in her occupational therapy assistant program at Bryant and Stratton College. We hired a babysitter and took a Lyft to the show, arriving before the gates opened.
The Dome’s muddy sound system threw me off as the concert began. Bruce’s opening number was “Lonesome Day,” but I couldn’t figure out the tune. I felt like an outfielder in baseball who can’t pick up the ball off the bat. The first song I recognized was “No Surrender,” and the sound quality seemed to improve as the concert wore on.
Bruce and the E Street Band played the anthemic classics, which I have been reliving through the miracle of YouTube: “Badlands,” “Backstreets,” “The Promised Land,” “Thunder Road,” and “Born to Run.”
Up in the nosebleeds, an exuberant middle-aged woman with long, dark hair kept bumping me as she swayed, stomped her feet, clapped her hands, and pumped her fists. She kept apologizing, but I didn’t care about the incidental physical contact. I appreciated the pure joy she displayed, and we formed a bond through our mutual love of the music.
After “Born to Run” finished with a flourish, we shared a two-word conversation—screamed into each other’s ears.
I turned to her and said, “Amazing.”
“Right!” she said.
I hardly go to concerts, and I can’t remember the last stadium concert I attended. It may have been when I saw Bruce in Phoenix in 2002 during The Rising Tour. I went alone to America West Arena during the sweltering heat of August.
A Syracuse woman posted on Facebook that she didn’t enjoy the show because of the behavior of the people around her. And I know a debate persists about proper concert etiquette. As for me, I love it when fans dance and shout the lyrics at the top of their lungs. I mean, if you can’t let loose at a rock concert, where can you? They’re not serving tea and finger sandwiches. I think your ticket should come with a warning like “buyer beware … this isn’t your living room,” and I sang many songs, my voice growing hoarse as the night continued.
Music provides bookmarks for people’s lives. Fans connect songs to significant moments in their lives. Bruce’s music sustained me during my darkest days when I was consumed by loneliness, shame, and self-hatred.
So when Bruce belted out the words to “The Promised Land,” I joined him and thousands of others in screaming:
Blow away the dreams that tear you apart,
Blow away the dreams that break your heart,
Blow away the lies that leave you nothing
But lost and brokenhearted …